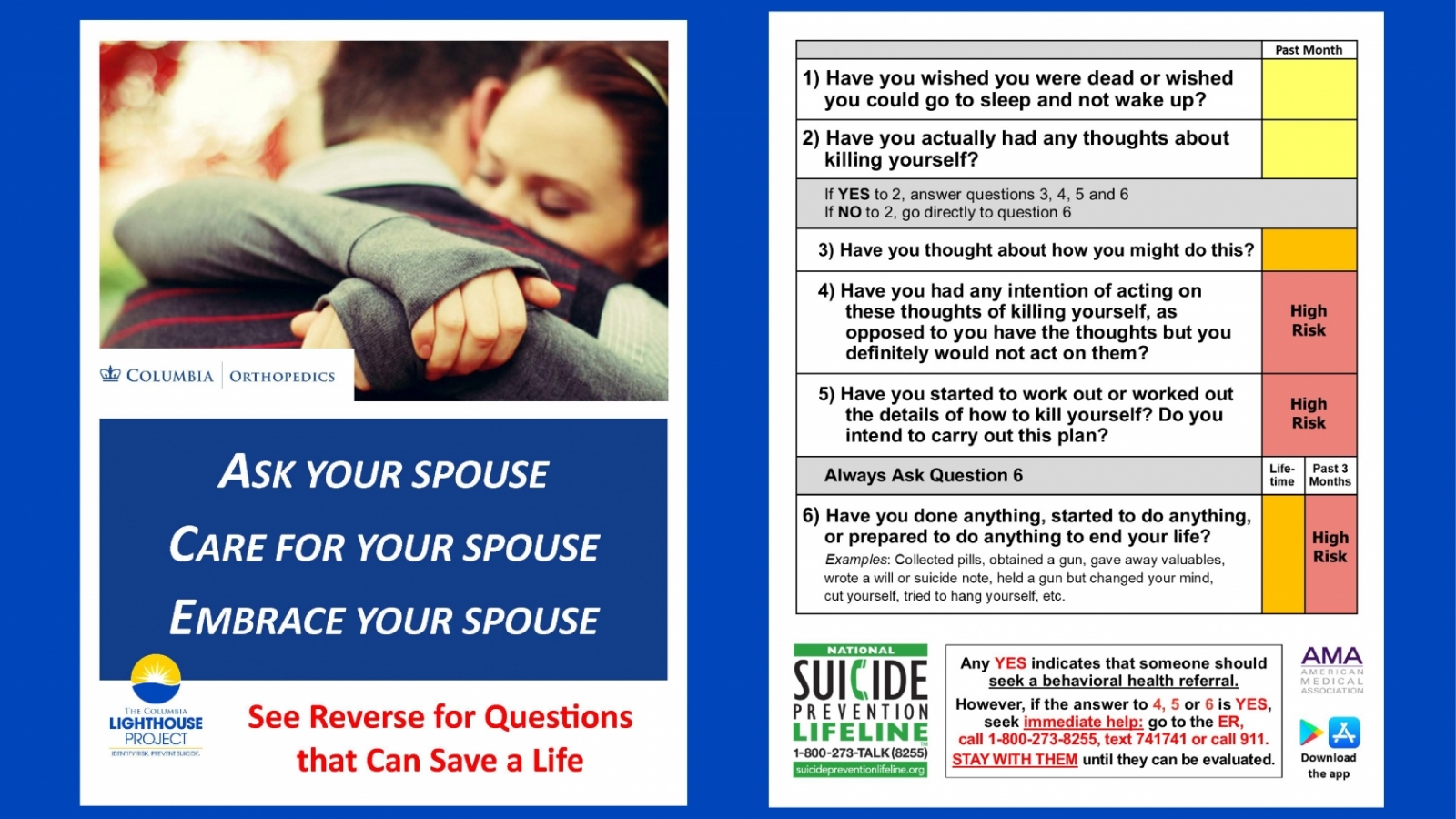
A Simple Set of 6 Questions to Screen for Suicide
The Columbia Protocol identifies people who are most at risk for dying by suicide and helps save lives.
Each year more than 700,000 people worldwide die by suicide—one person every 40 seconds—and many more attempt to end their lives. Suicide occurs throughout the lifespan and is the fourth leading cause of death among 15- to 29-year-olds globally.
Suicide, however, is preventable with timely, evidence-based and often low-cost interventions.
One such measure is the Columbia Suicide Severity Risk Scale (C-SSRS), a series of simple questions to assess the severity and immediacy of suicide risk that anyone can ask. The scale, translated into more than 150 languages, has been implemented in many settings, including schools, hospitals, college campuses, defense forces, fire departments, the justice system, primary care, and for scientific research.
Kelly Posner Gerstenhaber, PhD, professor of psychiatry at Columbia University, is the lead scientist of the C-SSRS along with researchers at University of Pennsylvania and the University of Pittsburgh. As director of the Columbia Lighthouse Project she continues to work with national and international governments and communities to integrate the C-SSRS into broader suicide prevention programs.
Psychiatry News spoke with Dr. Posner and Keita Franklin, PhD, co-director of the Columbia Lighthouse Project and former director of suicide prevention for the U.S. Department of Defense and Veterans Administration, about the C-SSRS and suicide prevention efforts.
How did the C-SSRS come about?
It’s been a great science-to-service story. Researchers from Columbia University, the University of Pennsylvania, and the University of Pittsburgh worked together in the first National Institute of Mental Health study of treatments to reduce suicide risk among adolescents. After identifying a gap in the field, we developed the scale in response to the need for a singular screening tool that could more precisely assess the full spectrum of thoughts and behavior and identify individuals at risk of ending their lives.
National agencies and programs including the CDC, FDA and “Zero Suicide” initiative have adopted the C-SSRS as the standard for measuring suicidal ideation and behavior. What explains this success?
One of the biggest obstacles to unified suicide prevention across public health has been the lack of a common language. The greatest impact of the C-SSRS has been to introduce a common detection method and make it accessible to all across public health. The C-SSRS allows everyone from teachers to parents to clinicians to use a simple set of questions to find those at risk and save lives.
We know that 50 precent of people who die by suicide have seen a primary care clinician in the month before they die. We need to treat suicide screening as routinely as we do blood pressure. In terms of reducing stigma, we know that asking these questions relieves distress for an at-risk individual. Large-scale suicide prevention hinges on the linking of systems and working across all public health sectors.
Is there evidence-based research that shows that the C-SSRS works?
More than 600 peer-reviewed studies have been published demonstrating its use in different populations and its validity. In a just-published study in Psychological Medicine of 18,000 psychiatric emergency patients, scientists in Sweden found that the C-SSRS screener "robustly" predicted death by suicide over one-week, one month, and one-year periods. Prior to the questionnaire, we didn’t know who to worry about. Individuals deemed at risk are routinely sent to hospital emergency rooms on a subjective basis. This approach has its price, as unnecessary referrals can shut down those who need treatment from getting it.
What results have you seen from the screening programs using the C-SSRS?
Screening in conjunction with other suicide prevention measures has already yielded positive results. States like Utah, where C-SSRS has been adopted as a policy tool, have seen reduction in suicide rates. Large acute care health care systems, such as Atrium Health, saw a 50 percent reduction in suicide across two states since implementing C-SSRS in 2019. These are just a few of the encouraging examples illustrating that when we are able to identify individuals at risk and connect them to the care they need, we’re able to save lives.
Dr. Franklin, you’ve helped to implement broad public health programming within federal government systems using the Columbia Protocol. Can you describe your work?
Navigating care within the military can be a challenge, in part because of the stigma of feeling weak or “less than” your colleagues if you ask for help. Dr. Posner and I collaborated to implement the C-SSRS within the U.S. Marine Corps and distributed the C-SSRS questionnaire to entire military communities—within the U.S. Air Force, Army, Navy, and the Reserve—engaging military spouses, coaches, and other gatekeepers. One of our biggest successes was that after U.S. Marine Corps incorporated the C-SSRS into of a broad public health strategy in 2014, suicides decreased by 22 percent within a year. Interestingly we also saw a reduction in other tragic issues like child abuse, domestic violence, and alcohol-related incidents.
What is your vision for where do we go from here?
The same way we moved people to wear seatbelts or stop smoking, we need to mobilize at every level to get people to know how to ask simple questions and respond to this public health crisis. The C-SSRS can be administered by anyone, anywhere. It is available as an app downloaded easily and accessed from a mobile phone. What’s become clear is the vital need to have a public health approach to find people where they work, live, and thrive.
For more information, visit:
https://cssrs.columbia.edu/
https://www.youtube.com/watch?v=csPPsstf2og&t=0s
https://www.youtube.com/watch?v=-ZwKBux1JoE&t=0s